

���������ζ���˨���ı��� Bland embolisation: BackgroundTAE�漰��Ѫ�����İ���������Ѫ���ڱ�����TAE�ڸ�ϸ���������е�Ӧ���ѳ���30�Marelli L, 2007����������ʽ��˨��ͨ������ʹ�������������������˨������PVA������ɣ�ͨ������Ϊ“Bland”˨������Ȼ����ļ����Ͳ����кܴ�ı仯����������Ŀ����ͨ�����������Ѫ�ܹ�Ӧ��ʵ������ȱ���յ�ϸ����������ǰ��ͬ��˨������Ӧ���ھ��ζ���˨���Ի��ƣ�transarterial chemoembolization TACE��
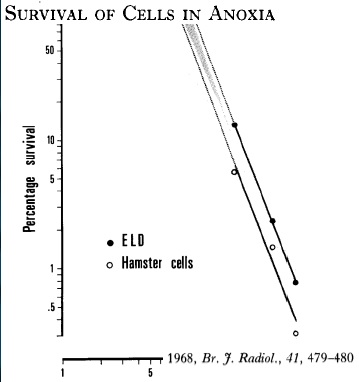
�����ǻ���ʱ�ᷢ�֣�������ĸζ���˨����TAE��bland embolization��������Ч�ԺͰ�ȫ����˵������˨����TAE����û�������е���ô� �ΰ�����˨����Bland embolization���ǻ���������ȱ���������Զ�����ϸ���Ի��ƻ���Ƶ������ԡ�Bland embolisation is based on tumor sensitivity to anoxia rather than cells chemo or radio sensitivity. �ΰ�ϸ�����������ڵĸΰ�ϸ������ͬ��ȱ��ʱ��ϸ�������ı仯��һ�������24Сʱȱ����ϸ��100%��������ֻ�����ǻ������������ڵİ�ϸ����ô��ʱ���ȱ����
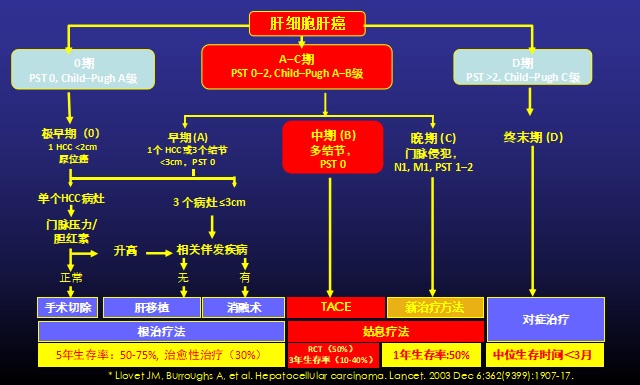
TAE�����ߵ�ѡ��һ����ԣ�TAEֻ�����и����������IJ����������ߡ�����BCLC�ּ�ΪB���Ļ��߿ɿ���TAE���ƣ�TAE��C�����ߵ������Ƿ�����������ޡ�Gbolahan O.B. 2017 Kishore S. 2017������ȻTACE��B�ڼ������Ƽ�Ϊ1A����Shah RP, 2011������������TACE��ȵ��ܷ��øߣ��ر��DZȽ϶�����Ч���о��ì�ܣ�һЩ����������TAE �� "bland - embolization" ��Llovet JM, 2002 Malagari K, 2010 Brown KT, 2016 Marelli L, 2007����������δ��֤����Ӱ��TAEԤ������ء�Thornton RH, 2009���� ���ڰ���TAE���ڵ����оֲ��������ƣ����ߵ�ѡ������Ի��ߵ��ٴ���Ѫ��ѧ��������������״̬���ι��ܼ����ٴ�ָ�꣬��ALBI(����-������)��CP (Child-Pugh)��MELD(��ĩ�ڸβ�ģ��)��ECOG(��������Э����)����״̬���֣����ڻ��߷ֲ��������Johnson P.J.2015 Levy I.2002 Guerrini G.P. 2018���������HCC�⣬��ǰӰ��ѧ����������Ѫ�ܽ��ʽṹ����·��λͨ���Ժ�ȷ���ž���ͨ����������Ҫ��Sieghart W.2015�����о����������������ٴ��ΰ����ڷ���ϵͳ(Barcelona Clinic Liver Cancer staging classification system, BCLC) B��ߴӸ������л�����������BCLC C��ߡ�Gbolahan O.B. 2017 Kishore S. 2017���� ����������UCSF����BCLC A�����߿��Խ���TAE��ά����ֲ�ʸ�Kishore S. 2017 Hodavance M.S.,2016����ͼ1��ʾ�˸���BCLC����ֲ�Ŀ������Ʋ��ԡ�
TAE ����֢����Ҫ���ǣ�TAE����û����ȷ���ų���; ����ʧ�����Ը�Ӳ��(Child-Pugh B8�����)�������ڸ�Ӳ�����ܵ�����>4 mg/dL���ߡ�Ѫ����>2 mg/dL���ž������ۺ����Բ�����Ϊ����Խ���֤�� TAE�Ľ���֤���ž���Ѫ�������Լ��١����������< 30 mL/min�����������ɡ����غϲ�֢��δ�����Ƶ�ʳ�ܾ������źι��ܱ�־�����ߡ�Raoul J.-L. 2011���� TAE �����Ͽ���
���������Ƶĺ���ԭ���Ǹ�ϸ��������Ҫ�ɸζ�����֧��Ѫ����������ʵ����Ҫͨ���ž�������˫��Ѫ����Kis B.2017 Breedis C. 1954 Gbolahan O.B. 2017������������ö���ͨ·��ʹ�õ��ܺ����������ѡ��Ӧ�����ĸζ�����֧���Ӹò�λ��ʼע��˨������ֱ����ѡ��������Ѫ�����͡�
������˨��(TAE)��Ŀ�������Ƹζ���Ѫ������������ѪѪ�ܡ���������ȷ��������Ҫ��Ѫ�ζ�����֧����ѡ����������������������ȵ��������Ч��������˨���ڽ��ĸζ�����֧����������ʵ�ʵ�ȱѪ�� ˨��ȱѪ�յ���ϸ��Ĥ���Ѻ��������Ӷ�����ȱѪ��ϸ��������Brown K.T., 1998����������Һ����Ͼ�����Ϊ˨������Vaidya S., 2008������ʹ��˨���� (�����������Ϊ40 ~ 120 μm������Rand T. 2005������Ը�����������Ѫ�����ܶ���˨�����Ƶ�һ����Ҫ���������������ڶ������������������̫С�����ܻ������е��·ζ���˨���� TAEҲ����Ϊ“Bland”˨������Ϊ���ӱ������߱����ƻ���Ƶȸ��ӹ��ܡ�
���ݼ����ڸ����ڵķֲ������Ʒ������Բ�ͬ�������Զ����Լ�����Ҷ���������ƻ�Ե����Լ�����Gaba R.C., 2017����ѡ���Ըζζ������ơ���Щ���߿�����Ҫȫ��������Zheng N. 2016��Coldwell D.M. 1989 Makary M.S.,2016 ������TAEͨ����������סԺ�����ﻼ���н��С�
micro-bland TAE�����������40-120μm����ȷ��˨��������������ĩ��Ѫ��
���߿��ܻ����˨�����ۺ���������Ҫ�ϴ�����˨���Ļ�����ͨ�������ء���ͨ���������Եģ�������˨����72Сʱ�ڳ��ָ�ʹ�����ġ�Ż�¡������衢ƣ�ͺ�/���ȡ�Castells A, 1995������ˣ�����TAE��TACE���ƵĻ���ͨ���ڳ�Ժǰ (ͨ���ǵڶ�������) סԺ��ҹ���Կ�����ʹ������Ӱ��ѧ��ʵ��������ͨ�������ƺ�4 ~ 6����ɣ���������Ч�����������Ӱ��ѧ����з��ֶ����Ѫ�ܻ���չ�����ƿ�����Ҫ������ơ�
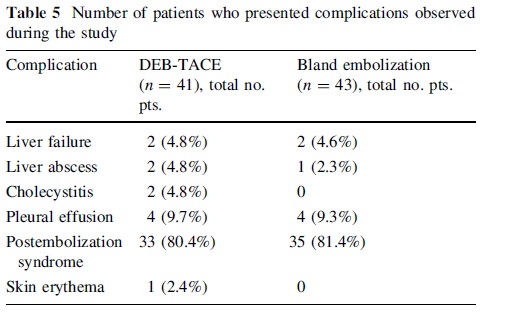
�������ط�����˨�����ۺ���(postembolization syndrome, PES)�������س̶Ⱥͳ���ʱ������뽡����֯ȱѪ�̶Ⱥ�DZ�ڵĸι�����ء�Wigmore S.J. 2003 Paye F. 1999�����������հ����ι���ʧ�����������ˡ��������ˡ���Ⱦ(ŧ��)�ͺ����ķ�˨��(����������δ�����ֵĶ�����������/��С˨������)��Chan A.O., 2002 Garwood E.R. 2013 Wu G.C., 2009 ������ǰ���˨������Ѫ��(�絨�Ҷ���������)����һ�����ա�Shah R.P.,2011��������ʹ������CT�����ͼ�������ȷ��������ȫ���ǣ�ͬʱ����ǰ�˨����Kluger M.D. 2014����
Χ�����ڹ���
������֮ǰ�����߿��ܻ�������������Ԥ���Կ����أ��Ը��Ǹ��������Գ������Watchmaker ���������˸�˨��ǰԤ����Ⱦ�ı�Ҫ�ԣ���������������������������Oddi��Լ����õĻ����а�ȫ�ؽ���������Watchmaker J.M.2018��;Ȼ�������ڼ�����������Ԥ������Լ�����ܸı�Ļ��ߣ������Ⱦ�ķ������Ը��ߡ�Song S.-Y. 2001������ˣ����������ƺͳ��������ܶ���Щ�������档���磬Khan���˷��֣��Ը�ŧ���γɸ�Σ���ߣ����ζ�������ǰ3�졢����17��ڷ�400 mgĪ��ɳ�ǿ���ЧԤ���ò���֢��Khan W. 2011������һ�ַ�����������ǰÿ��ʹ��������ɳ�Ǻͼ�����2�죬����˨��ǰһ�������1�㡢2���11������ʹ����ù�ؼӺ�ù�صij������������ʹ��2�ܡ�Patel S.,2006����������ǰ���ǰ���ˮ��״̬��ֹ�¡����鰷����̴���һЩ����ʹ�õ������ɺ��⻯�ɵ��ɡ�
���������ˮ�֡���ʹ�Ͷ��Ŀ����Լ��ȶ��ĸι��ܼ���dz�Ժ�Ĺؼ�����PES��˨����������IJ���֢������Ϊ���ϸ�����ʹ�����ġ�ƣ�͡����ȡ���ת��øѪ֢�ߵ�����Ѫ֢��Wigmore S.J. 2003 Paye F. 1999 Castells A. 1995������ͨ����������72Сʱ�ڷ��������ڴ����������������Եģ�����7��10������ȫ���ˡ�Castells A. 1995���������������صij����ҩ�������飬�ڻ�ø��ɿ�������֮ǰ����Ӧ��ȡ���ڲ����IJ�ͬ��Brown D.B., 2006����������ԣ��е����쳣��������Ԥ��Oddi��Լ�������ϰ���ʷ�Ļ���Ӧ����ʹ�ÿ�����2�ܡ�Khan W. 2011����Ӧ��ѭ�ʵ���Χ�����ڿ�������ָ�ϡ�Pudusseri A.2014 Patel I.J. 2012����4-6�ܺ�������Ӱ��ѧ��ʵ���Ҽ�飬�˺�ÿ3-6���½���һ����ã����������Ƴɹ�����⼲����չ��Gbolahan O.B. 2017 Haste P. 2018����CT��MRI��֤ʵ����������Gaba R.C. Radiol. 2017����
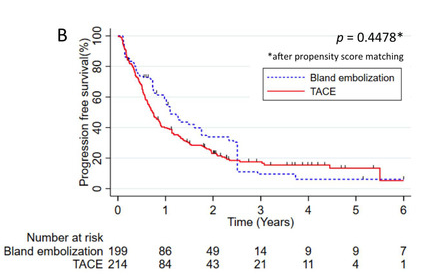
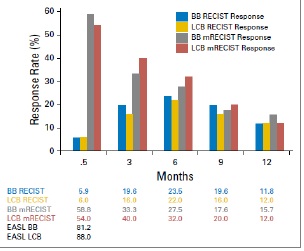
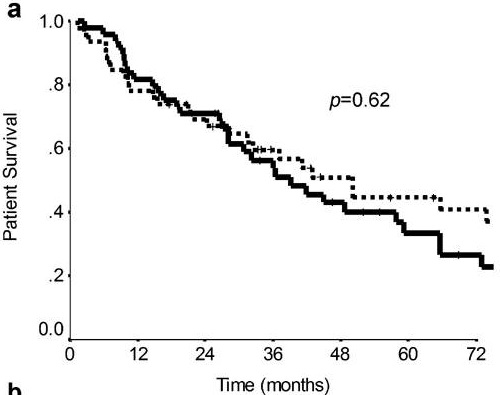
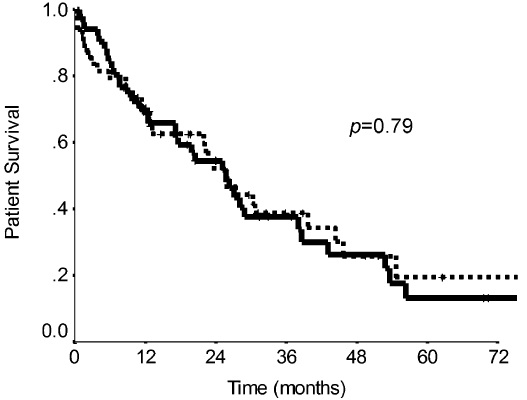
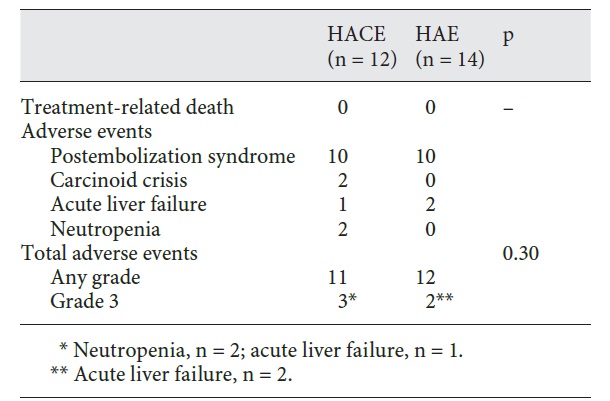
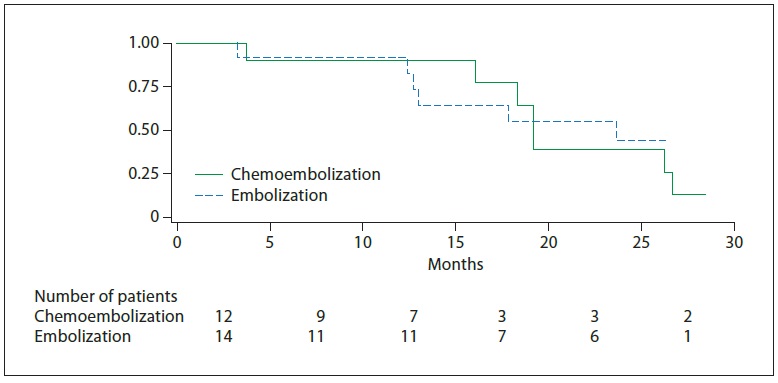
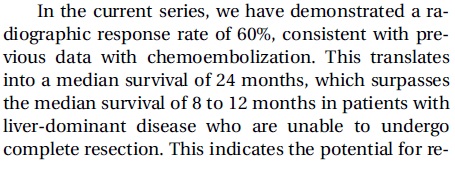
Locoregional Therapy Approaches for Hepatocellular Carcinoma: Recent Advances and Management Strategies �����ζ���˨���������Ԥ�� ������������ԭ���Ը�ϸ����(HCC))�����з��������õ����á��ٴ��о���ʾ��TAE��TACE�ȽϷ���Ч�ԡ����ڻ�������˨�������Ƹ�ϸ������HCC���е����ã�Ŀǰ������ȷ�Ľ��ۡ��Ƚϻ��߾���������˨�����ƣ�TAE���;���������˨�����ƣ�TACE���Ŀ۷�Ӧ�ʡ����Ժͳ���Ԥ�������ó����ۡ� һ��ع��Ե�������265�����������Ľ��ܵ�һ��TACE��TAE���Ƶ�HCC���ߡ�������ǰ��¼�ٴ�������ѧ���������ڵ�һ�����ƺ�ʹ�ø�����ʵ��������Ӧ��������mRECIST������������ѧ��Ӧ��Roth 2021�������ƺ�����֮�������ԣ���չ������ֲ������е�����ʹ����������ƥ�䣺 86�����ߵ���˨�����ƺ�179�����߽��ܣ�����44��ҩ��ϴ�����135���͵����ƣ�89.8%�Ļ���������ƽ������Ϊ65�ꡣ90.9%�Ķ�ͯPugh����Ϊa�Ļ��ߺ�84%�Ļ��߳��ָ�Ӳ���� ���������������Ʒ���֮���AE�����ʣ������ι���˥�ߣ�û���κβ��졣TACE����ȫ�۷�Ӧ�ʣ����Ʊȣ�OR��= 8.5 (95%�������䣨CI����2.8-25.4����������������أ������ܷ�Ӧ�ʣ�OR=2.2��95%CI=0.8-5.8�����ء���TACE��TAE֮����������ڣ�p = 0.3905������չ�����ڣ�p = 0.4478��������ֲ�����ڣ�p = 0.9020��֮��û�в��졣��TAE��ȣ�TACE����ߵ���ȫ���䷴Ӧ����أ�����������䷴Ӧ����չ�����ں���������û���κ�Ӱ��
Ŀǰ�������ٴ�����ϵͳ������Ԥ��HCC���������ƺ���������ڡ���չ�����ںͲ����¼�������Okudaϵͳ�����֢������ƻ�(Cancer of the Liver Italian Program, CLIP)���֡���۸ΰ�(Hong Kong Liver Cancer, HKLC)����ϵͳ�Ͱ��������ٴ��ΰ�(Barcelona Clinic Liver Cancer, BCLC)�������Grieco A.2005 Yau T. 2014���Լ��й��ΰ����ڷ��������ض���Ԥ�������У��������ɡ��δ�����������ɢ������״̬��HCC����������������ء�Grieco A.2005 Tsochatzis E.A.2014 Llovet J.M., 1999 Ni J.-Y. 2018�����������Ʒ�Ӧ�Ľ����2010�����ġ�ʵ������Ч���۱���(mRECIST)��Kim M.N. 2015����
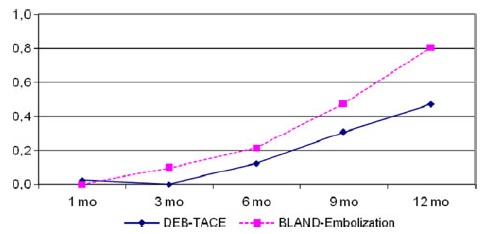
�����֧��������ȣ�TAE���ƴ�����������������桾Gbolahan O.B. 2017 Llovet J.M. 2002����Tsochatzis�ȡ�Tsochatzis E.A.2014�������˶�6��Ƚ�TAE��TACE�����������������ͷ��������û��һ��������ʾ�����������������졾Tsochatzis E.A.2014 Meyer T 2013����Lee���ˡ�Lee E.W.2017���ܽ��������о���֤�ݣ���ʾ3�������ʡ������¼���RECISTӦ�����������졾Lee E.W. 2017 Kluger M.D.2014 Massarweh N.N.2016 Brown K.T.2016������Ȥ���ǣ�Kluger�ȡ�Kluger M.D.2014�����֣���TACE������ȣ�TAE��������ֲǰ��Ҫ�ٴ����ƵĿ������������͡����2009��һ��Ƚ�ҩ��ϴ���龭��������˨��(DEB-TACE)��TAE�Ķ�����RCT���֣�DEB-TACE�����������չʱ���������ƣ������������ޱ仯��Malagari K. 2010����
����֤�� Outcomes of Transarterial Embolisation (TAE) vs. Transarterial Chemoembolisation (TACE) for Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis ����˨������������շ���ȱѪ����������ϸ����������Ҫ���أ���TAE˨��ȷʵ�����˻��Ƶķ��ü��䲻�����ԡ�Chuang V.P. 1981 Tsochatzis E.A. 2013�������Ӧ���������ʵ�ѡ��Ļ����ṩTAE��
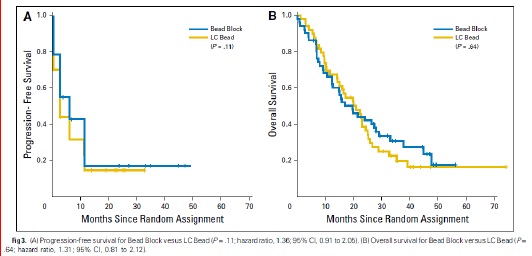
�о��Ѿ�֤��TACE�����֧����������������档��TAE��û�������ıȽ�����;һЩ�о�����TAE�����淴Ӧ�ϲLlovet JM, 2002������Ȼ���ͷ������ݱ���TAE�����TACE���з���Ч�ԡ�Marelli L, 2007������2009���һ��Ƚ�DEB-TACE��TAE�Ľ���ǰհ�����������DEB-TACE��ļ�����չʱ��(TTP)�ϳ�����ȫ����ĸ���ٷֱȽϸߡ�Malagari K, 2010�������������һ���о��������ڱȽ�bland˨����DEB˨��ʱ���������⡢��չ������(PFS)����������(OS)���졾Brown KT, 2016������ˣ�TAE��TACE����������HCC������������ƽ�ȵģ��в�̫���������ȷ���о���
��Ҫԭ����ҽ�ƻ�����ҽ�����˷�����о�ȱ���Ӵ���ʽ�֧�֣���TAE�ǹ�ʱ�IJ�Ǯ�IJ�Ʒ�����Ӵ��ʽ�ij�������֧���������о��������о�����Ҫ��������ҽ���⸶������Ҳȱ�ٶ��������������о���δ��������Ҫ���һ��𣬴��ƻ�������ܵĽ�����¼�������˨�����Ƴ�Ϊ��ʷ�� �����ζ���˨����Ӧ֢֮һ����ϸ���ΰ� 
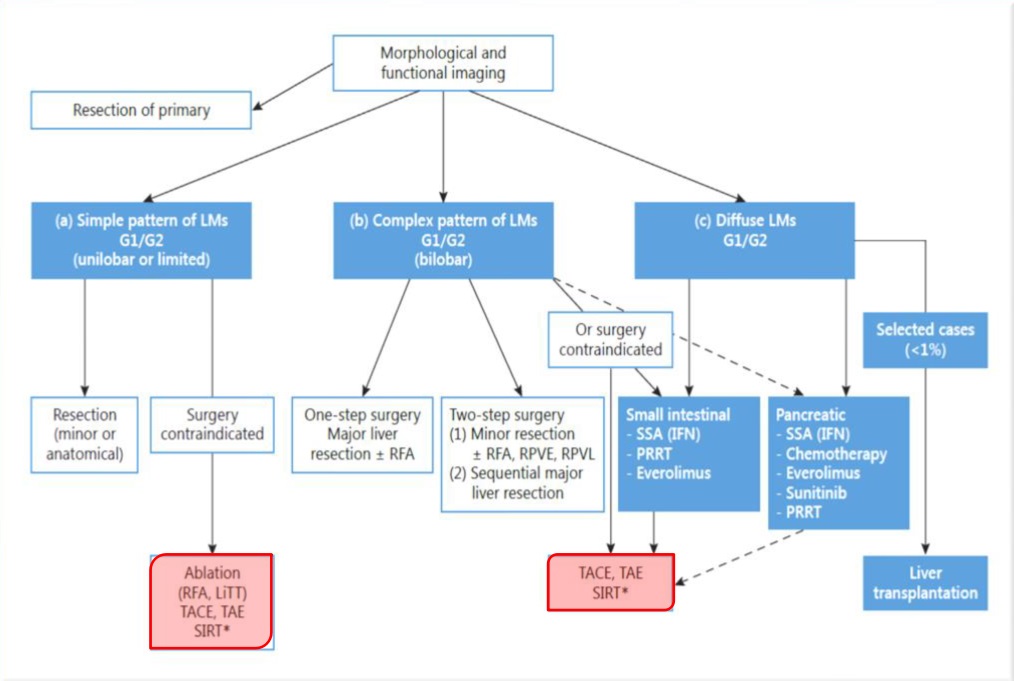
����ΪTAE������Ӧ֢�����ζ���˨����Ӧ֢֮�������ڷ���������NETs�� ��Ҫ�ʺϻ��� - G1/G2 NET��GEP-NET��θ�����ڷ������� - Ki-67 �� 10% - Liver dominant ʲôʱ����Կ���NETs��˨������ - ����֢״����ۺ����� - �����������ɣ�Debulking�� SSA���ƺֲ�����Ӧ�þ��������Ӧ���Է�ֹ�����Ի����ڷ����������Σ���ر����г��ڷ����������͵���ۺ������������������ڸ��࣬�ֲ����ƿ�����Ϊ�ǹ�������ȫ�����Ƶ�һ��ѡ� 
 Hepatic neuroendocrine metastases: chemo- or bland embolization?
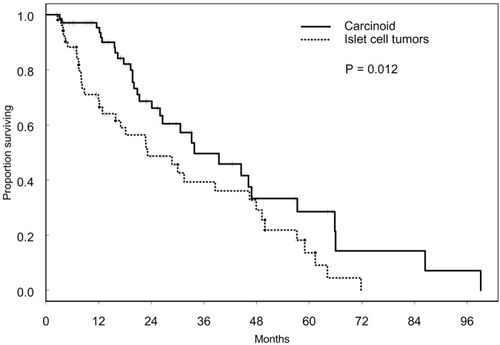
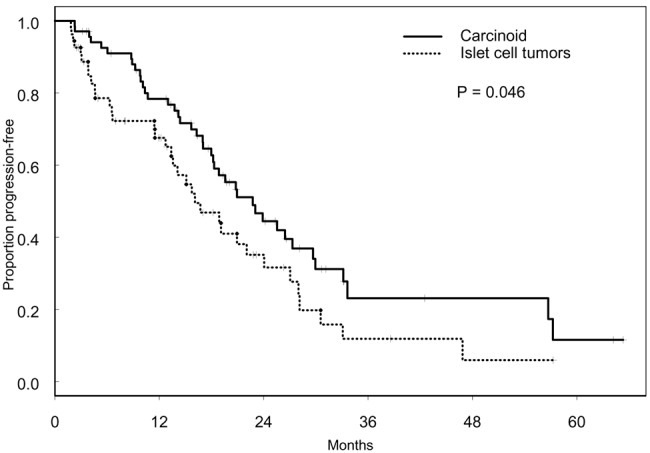
Hepatic arterial embolization and chemoembolization for the treatment of patients with metastatic neuroendocrine tumors
Maire F.a · Lombard-Bohas C.d · O’Toole D.a · Vullierme M.-P.b · Rebo
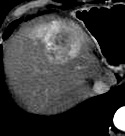
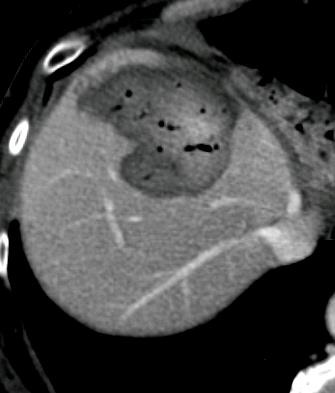
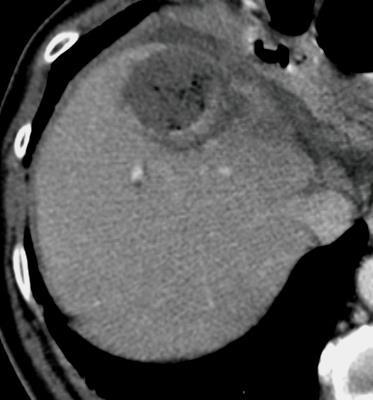
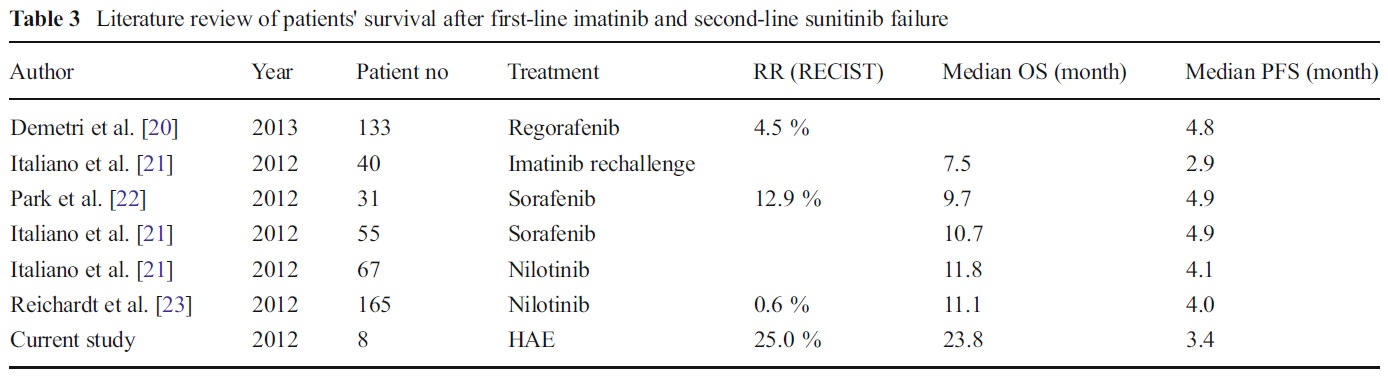
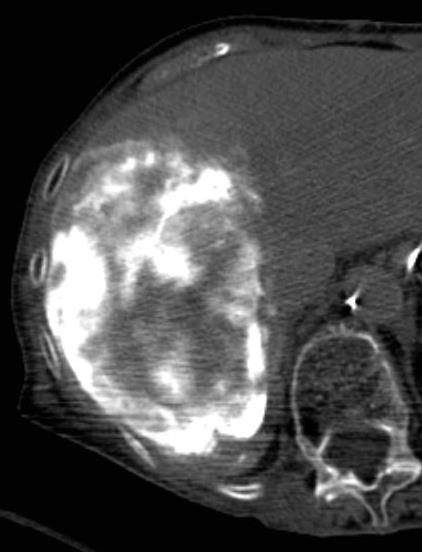
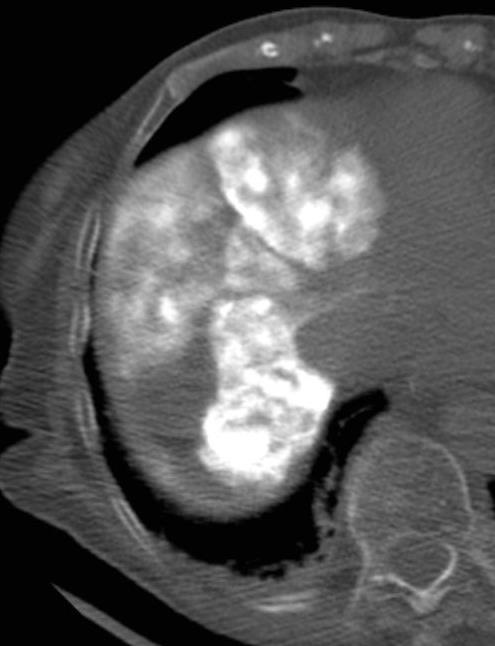
   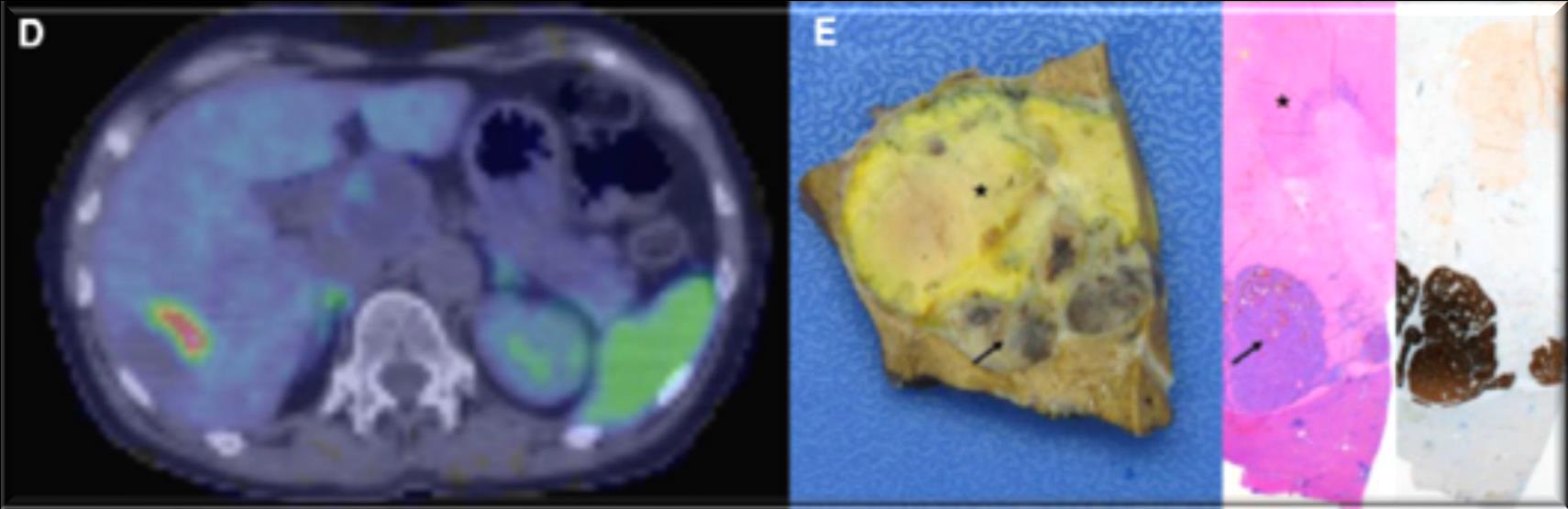 ��ͼƬ��˳�����������ԭ�ģ�     Histologically-Proven Efficacy of Bland Embolization in a Patient with Net Liver Metastasis TAE ��Ӧ֢֮����GIST
- Sunitinib (second line)
 
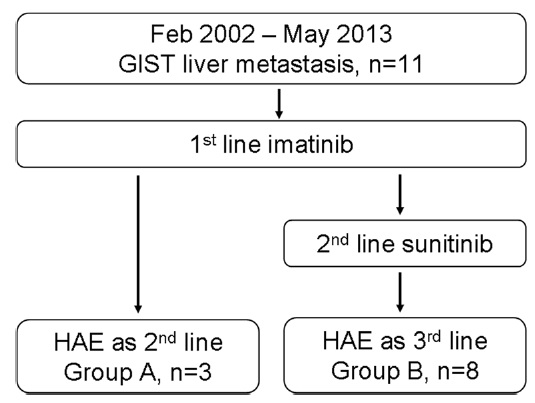
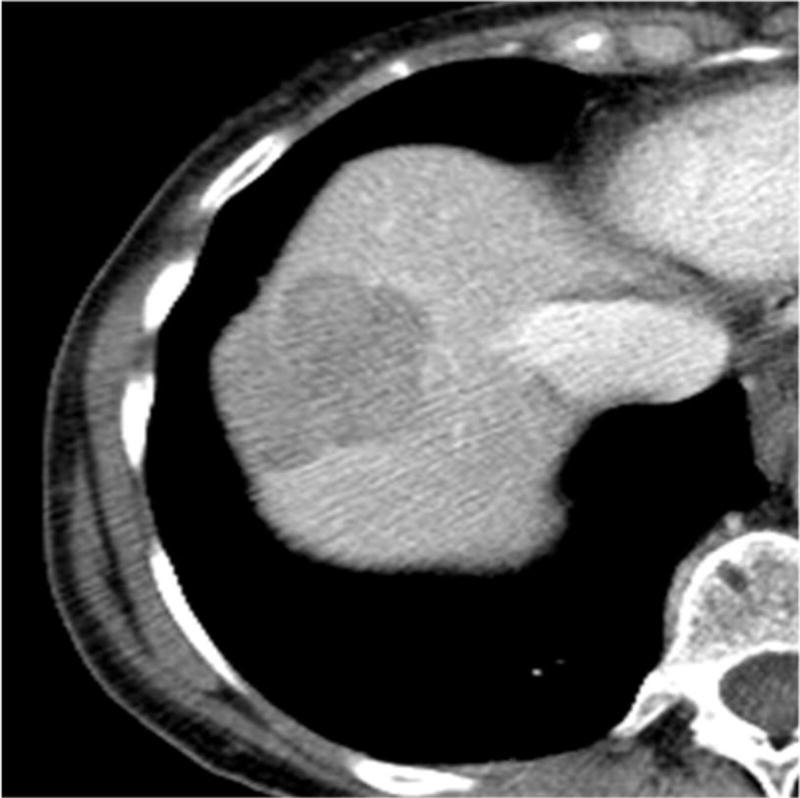
Hepatic artery embolization for liver metastasis of gastrointestinal stromal tumor following imatinib and sunitinib therapy.
Bland embolisation: GIST
����
Not be blind, Try to be bland!
Ki-67����ϸ��G1��S��G2��M�ڳ��ֵĺ˿�ԭ���������˥�ڶ̣�����ȷ��ӳϸ������ֳ���ԣ��ѹ㷢Ӧ���������������ֳ���Բⶨ���������������֢�ͼ��ر仯�Ķ�Ӱ�죬���¾����ڵĻ����ں������ڣ���״��Ƥ�����ϲ�ϸ��ki-67�������ӡ�
�����黯��� �����黯����Ӧ������ѧ����ԭ��——��ԭ���巴Ӧ������ԭ�뿹�������Խ�ϵ�ԭ����ͨ����ѧ��Ӧʹ��ǿ������ɫ����ӫ���ء�ø���������ӡ�ͬλ�أ���ɫ��ȷ����֯ϸ���ڿ�ԭ�����ĺ͵����ʣ���������ж�λ�����Լ��������о�����Ϊ������֯��ѧ����(immunohistochemistry) ������ϸ����ѧ���� (immunocytochemistry) �����黯Ⱦɫ���� ����֯��Ƭ�������ݶȾƾ���ˮ�����������ο�ԭ��Һ������PBS����Һ��ϴ������1:50ϡ�͵�ki-67�����������·���1h,���������������ø�Ŀ�������������·���45min��DBA��ɫ��Mayer��ľ����Ⱦ
Ⱦɫ����ж�
���غ�ɫ����λ��ϸ�������ж�Ϊ����Ⱦɫ�����������Beesley�ּ�������������ϸ�����ı�����Ⱦɫ�����Ϊ�ļ�
ͬʱ���������ʵķ����趨Ϊ��1.�����ʣ�ָһ����һ�����ϵ�����Ⱦɫ�����ٷ�����2.ǿ�����ʣ�ָ2���Լ�2�����ϵ�����Ⱦɫ�����ٷ���
�ڲ�ͬ��ϸ�������Ա�����
SSA���Ƽ�� �����������������ƵĻ�����
Pasireotide��һ�����͵��������������Ŀǰ�����з��У������ðе�Ϊ SSTR1��2��3��56
��������Ӧ������
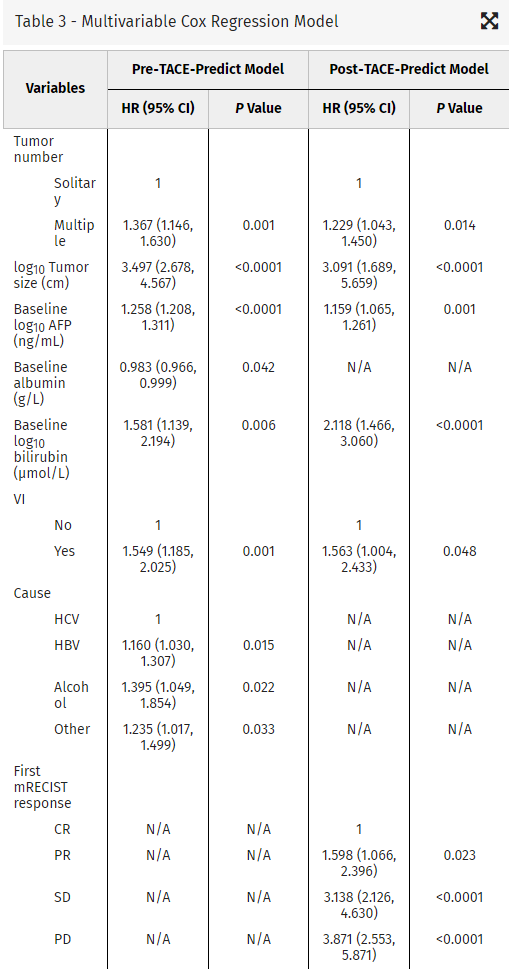
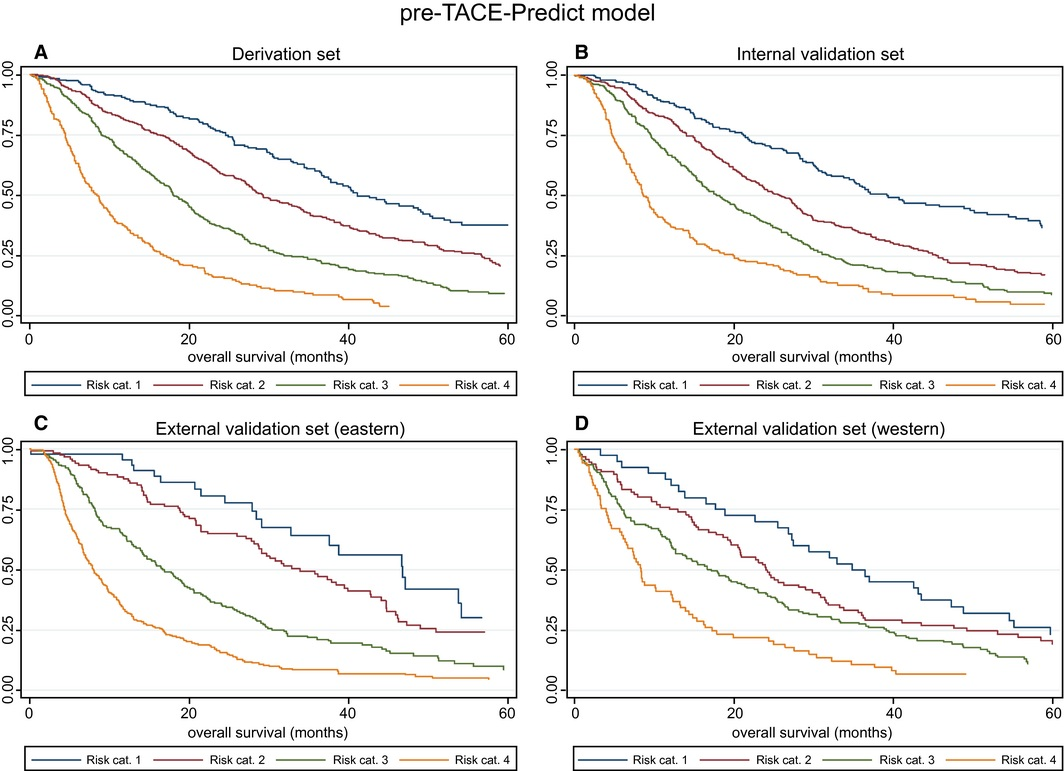
��TACE�ķ�Ӧ�����������ʶ���Ԥ������
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||















 |
���ֲ��䶯����ǿ��������
��ȷ��������û�з��ֵ�������Ѫ
CBCT ���������������� 90% vs DSA 67%
CBCT ����������Ѫ������������ 93% vs DSA 55%
 |
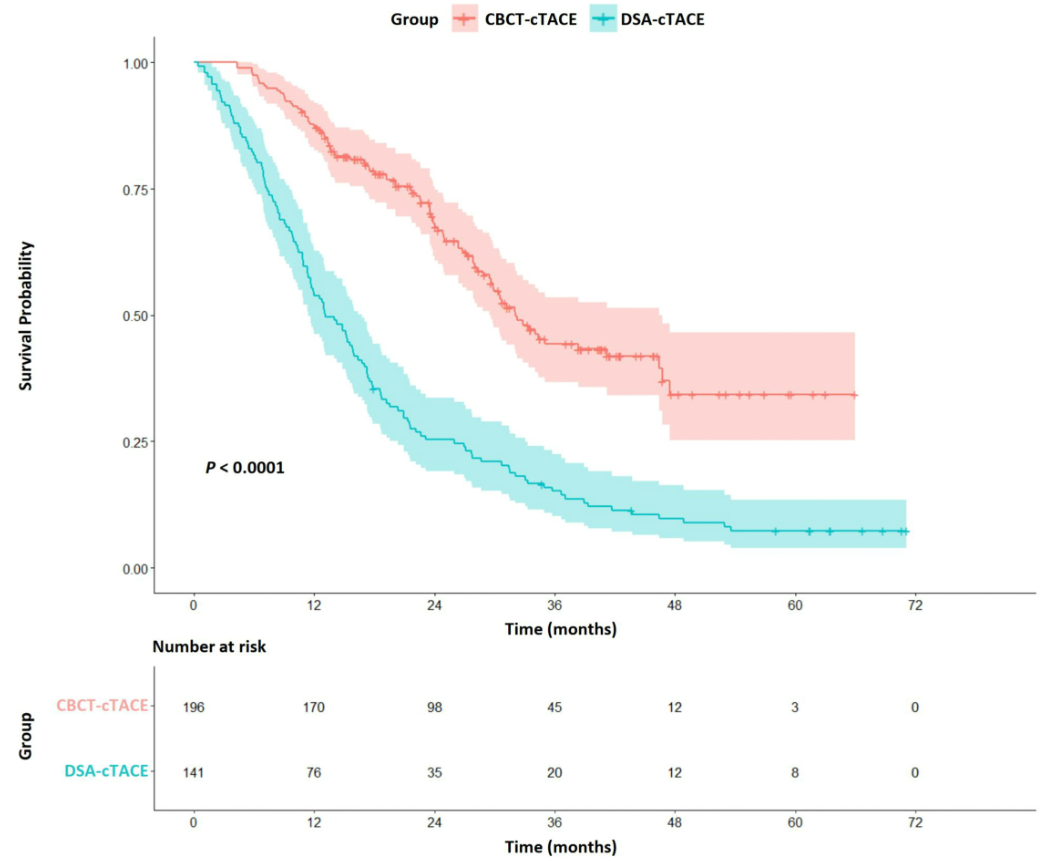 |
�봫ͳ��DSA��ȣ�ѡ����cTACE����CBCT��AFD�����ɸ�����������HCC���ߵ�������Ӧ���ӳ�OS��
������CBCT�ͷ�ӦԤ��
 |
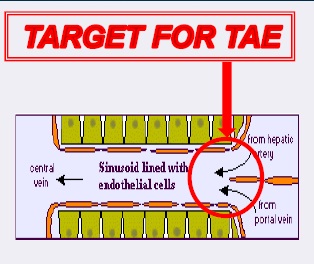 |
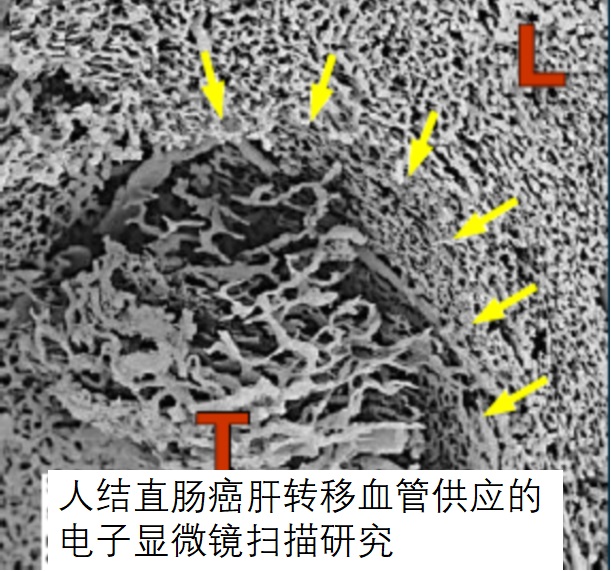
| �ζ���˨���İе� |
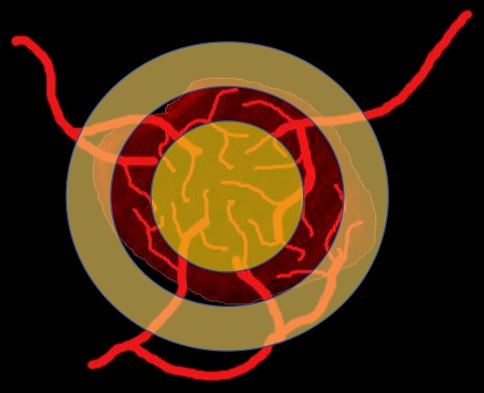
���ν�ڵĶ���Ѫ�����Ǵ��ڵģ���ʱֱ��������Ѫ�ܽ�ͨ����Ϊ�������ǣ���Ҫ�Ǹ�ת�ư�������Ѫ��ֱ���������ӡ�
 |
|
“Such embolization of tumors can be obtained only with the use of calibrated TGMS of adapted caliber
to avoid proximal occlusion”
|
| ����������˨��ֻ��ʹ�þ�У������ھ���TGMS���Ա�����˱�������Ҫ��ѡ��˨�� |