

什么是理想的血管造影技术(opimizing angio technique)?先说阴性血管造影的临床随访结果
Kim - 2009 Kor J Radiol; 10:384 血管造影诊断消化道出血的阴性结果可能是假阴性
再说活动性造影剂外溢的预测因子 Predictors of Active Extravasation
Lee - 2012 Can J Surg 55: 382 应该不止于此,还应包括从发病到血管造影的时间,患者凝血功能障碍没有得到纠正....,
知道从哪儿开始寻找出血
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 |
 |
|
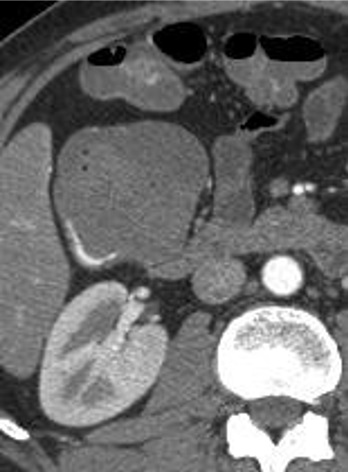
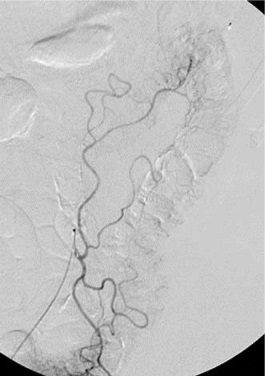
Extravasation in Cecum
|
Angiodysplasia
|
理想的技术(Optimal Technique)
- 导管位置固定 Have catheter well seated
- 注射足够的造影剂 Inject enough contrast
Proper rate to fill vessel without inflow 合适的注射速率充盈血管
充足的容量能够发现造影剂外溢 (通常4-5秒)Adequate volume to be able to identify extravasation (usually 4-5 seconds)
- 胰高血糖素和憋气 Glucagon, breath holding
- 充气 Air insufflation
- 确定解剖部位覆盖 Make sure to cover the anatomic distribution
- 选择性注射 Inject selectively
- 如果出血没有发现再注射 Re-inject if bleeding not seen initially
 |
 |
 |
 |
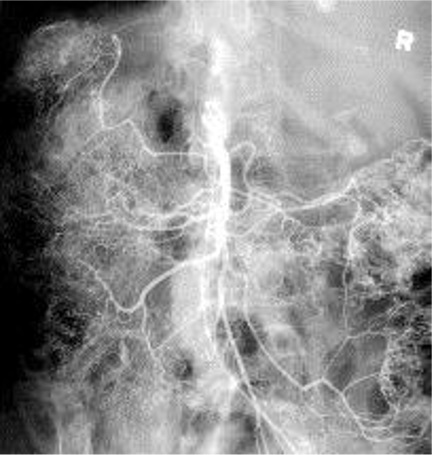
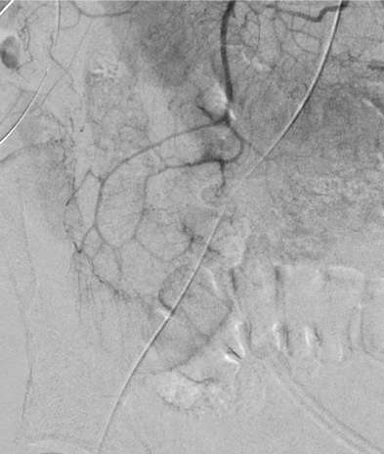
| 出血点险些出覆盖范围(最下方) | 右结肠动脉出自腹腔动脉 |
投照没有足够低的中心 Failing to Center Low Enough
 |
 |
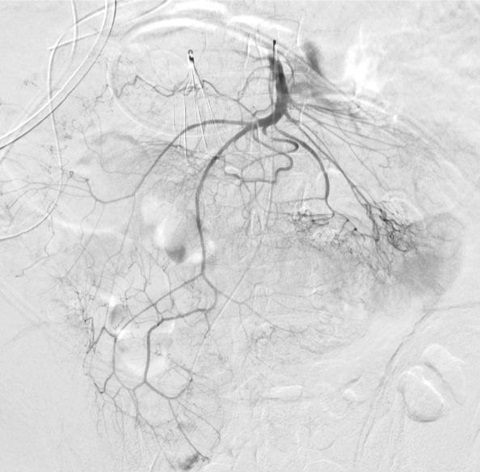
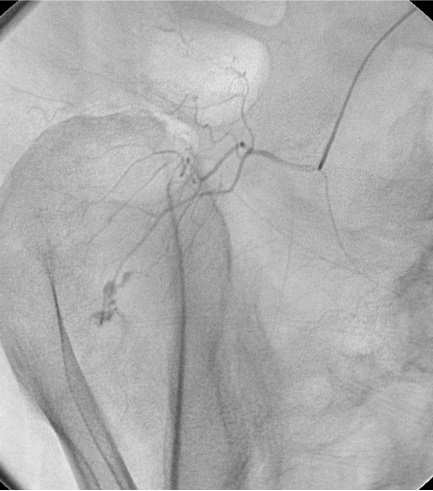
Value of Selective Injection
 |
|
 |
 |
| Non selective injection from SMA trunk | Selective injection in ileocolic branch |
Value of Selective Injection
 |
 |
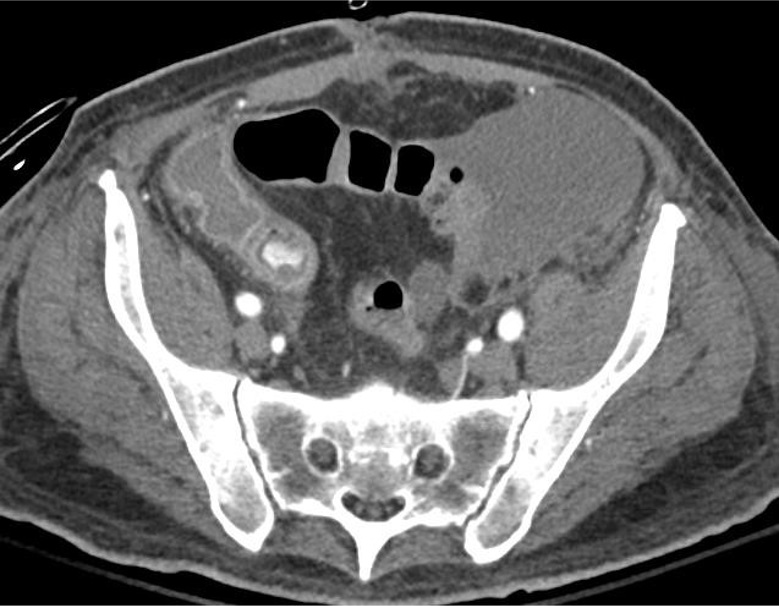
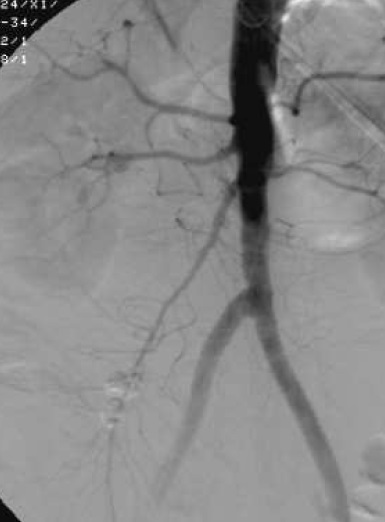
| 造影剂外溢? | Yes! |
1. 血管造影时必须要做的,特别是选择性GDA
2. 不要忘记进行SMA
3. GDA 采集需要从上到下
4. 若DSA采集时间长,+ 透视
5. 征询内镜医生止血夹的出血位置
6. 抑制肠蠕动(glucagon/buscopan)
7. 激发出血*
*Johnston et al. use of provocative angiography to localize site recurrent GI bleeding. CVIR 2007: 30, 1042 -6
 |
 |
 |
|
| 腹主动脉造影未见明确造影剂外溢 | 血管造影时必须要做的,特别是GDA |
 |
 |
 |
|
Initial SMA angio
|
Repeat SMA angio 15 min later
|
激发血管造影(Provocative Angiography)
间歇性出血的潜在解决方案
全身给药或选择性靶血管给药
目标:
防止血栓形成用肝素
血管扩张用硝酸甘油或妥拉苏林
出血部位的溶栓用溶栓剂
73例下消化道出血,21例应用激发血管造影(Used in 21 of 73 lower GI bleeds)
定位诊断增加32%-68%(Diagnostic yield increased from 32% to 69%)
阴性血管造影降低27%-16%(Negative arteriograms decreased from 27% to 16%)
Rosch – 1988 Semin Intervent Radiol; 5:10
 |
 |
 |
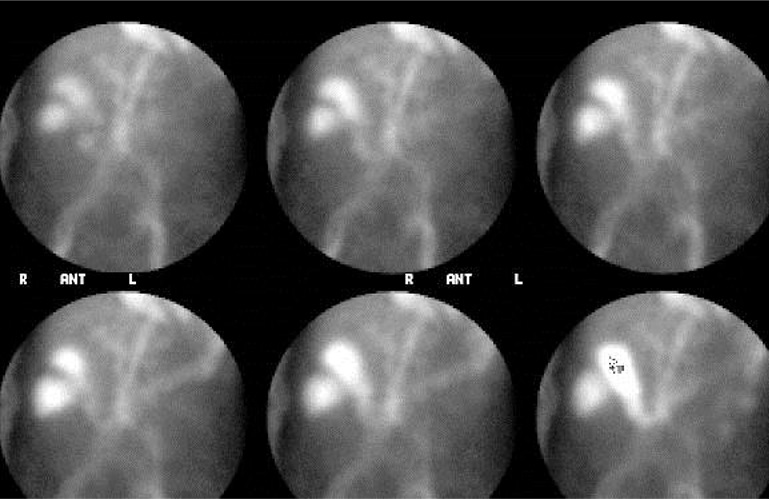
| Pre tPA | Post tPA | Post tPA |
34下消化道出血病人,36次激发血管造影(34 pts, 36 provocative angiograms)
11 (31%) 可见造影剂外溢 (- visible extravasation at angio)
10 of 11 出血成功进行栓塞 - hemorrhage controlled by embo
没有出血并发症 No hemorrhagic complications
Kim - JVIR 2010 ; 21 : 477